
El Paso to Phoenix, 11:30 p.m., cruising at 12,000, we could barely hear the radio calls from all the laughter in the cockpit. It was the second leg of three, after taking delivery of our newly acquired Twin Comanche in Dallas. The winds aloft were warmer than normal.
We were positively giddy that neither the heater nor jackets were needed. That wasn’t the only thing we found funny. The infinitely black night sky. The hilarious way the Milky Way flung itself across the night, like a Jackson Pollock brush stroke. The way “Pollock” sounded almost like “polyp.”
We spent another 20 minutes unable to contain ourselves over our sudden and persistent farting attacks. When radio calls did manage to pierce our howling good time, imagining what the person connected to the disembodied voice looked like just incited more eye-watering, belly rolls of laughter. Just two guys in the cockpit acting ridiculous. Or was it?
The good times continued while ATC kept us at 12,000. Amidst all the fun, we forgot to brief the approach. At 15 miles from Hamek, we were suddenly cleared for the KPHX ILS 25L approach, with instructions to cross Hamek at 4,000 feet.
Cranking over to a 1,500 fpm descent to make the crossing restriction was the last funny thing we did.
Passing through 9,000, a noticeable behavioral change overtook us. What was funny suddenly became annoying. At first I thought the change in attitude was from needing to focus on quickly executing a high rate descent while briefing the approach and entering an unfamiliar airport environment.
Once on the ground, I began to consider hypoxia as the cause of our at-altitude shenanigans. Gone was the laughing attack, my sense of fatigue and the gas. My vision seemed to regain its sharpness. I asked my copilot how he felt. His observations concurred with mine.
After an L39C Albatros pilot had a similar experience at a cabin pressure altitude of 12,000 feet, he too submitted a report to NASA’s Aviation Safety Reporting System, also known as a NASA report.
“Flying in a pressurized cockpit at 17,000 feet, I noticed I was focusing very intensely on the gauges, more than usual. I checked cabin pressure (two separate gauges installed), and both were reading just over 12,000 feet. At this point, I wondered whether or not my increased focus on the instruments might have been due to hypoxia.”

The Breitling Jet Team flies L39C Albatros jets. (Photo courtesy Breitling)
Fast approaching cloud buildups, the pilot chose to cancel IFR and attempt a 180 back into VMC rather than continuing to wrestle with attaching his O2 mask and flying on instruments. When he finally did attach the mask, he still got no relief.
“The valve in the mask seemed to be opening for only the first part of each inhalation. I panicked, realizing that I was probably becoming more hypoxic and my oxygen wasn’t working.”
The L39 pilot’s hypoxia symptoms were fixation, poor decision-making and panic. Ours included gas and uncontrollable laughter.
A Beechcraft Bonanza pilot reported different symptoms altogether in his NASA report.
This pilot wrote of “cruising for about four hours at 12,500 feet uneventfully. When I announced to Center that I would commence a VFR descent is when things went awry.”

Beechcraft Bonanza
When Center handed him off, the pilot was unable to dial in the correct frequency.
“My attempts at contact went nowhere, and somehow I was unable to return to my previous controller. This seemed incredible for a pilot with my level of experience.”
For him, hand flying the airplane was not a problem. But performing the simplest mental task became impossible.
Symptoms
Hypoxia is a curious ailment, partly because of the wide array of symptoms associated with it. Only some are discussed in conventional flight training. Those most often mentioned include headache, giddiness and reduced mental capacity. But there are many other symptoms, including gas, shortness of breath, tachycardia and cyanosis (the bluing of a body part from lack of oxygen).
A C-182 pilot and his passenger experienced a cyanotic event, according to their NASA report. They were cruising at 13,000 feet for about 40 minutes when the passenger complained that his hands were turning blue.

Cyanosis of the hand in someone with low oxygen saturations. Photo By James Heilman, MD
{kind=link}
“However, there were no other signs of hypoxia,” the pilot wrote in his NASA. “At that time I requested descent to a lower altitude, fearing hypoxic conditions were setting in.”
“Setting in” is an understatement. By any definition I researched, cyanosis is considered an end stage symptom of hypoxia. After that, the progression tends to be unconsciousness and death.
For most GA pilots, hypoxia’s onset is usually subtle. It didn’t occur to my copilot or to me that we had a problem. All we knew was over time every word, every image, every sound evoked laughter.
It wasn’t until the L39C pilot realized he had been fixating for a long time on his aircraft’s instrument panel that something might be amiss. And the Bonanza pilot flew for four hours at 12,500 feet before the ill effects overtook him.
I researched more than 100 reports in the ASRS database. Only one instance of “sudden onset” was recorded.
A Gulfstream III was flying at Flight Level 430 when the jet’s owner entered the flight deck. He accidentally banged his head against the emergency electrical gang bar, knocking all electrical power offline. The cabin depressurized. The flight crew and other passengers successfully donned oxygen masks, but the owner didn’t. Hypoxia rendered him unconscious in seconds. Talk about one of those times when not even being the boss can protect you…
Why does hypoxia affect some people one way and others another? Could the differences in reaction correlate to age? Weight? Physical conditioning? It’s hard to know.
The Bonanza pilot reported that he was a 73-year-old in excellent health who never smoked or drank. I was in my early 30s, lifted weights and rode a bicycle regularly. But I’d also just kicked a decade-long cigarette habit the year before. My copilot was in decent shape, in his mid-20s, didn’t smoke, but drank occasionally.
When it comes to hypoxia, here’s what we do know: How well a person’s lungs take in oxygen, how well a person’s hemoglobin binds to atmospheric O2, and how well one’s circulatory system distributes oxygenated blood throughout the body determine how severely hypoxia strikes.
Do you know what your oxygen intake, your hemoglobin uptake or your blood distribution rates are? You can’t. They aren’t constants, like your blood type.
Prevention
So how can we guard against hypoxia? Thankfully, there are two constants that tend to protect us: One, federal regulations and two, Boyle’s Law.
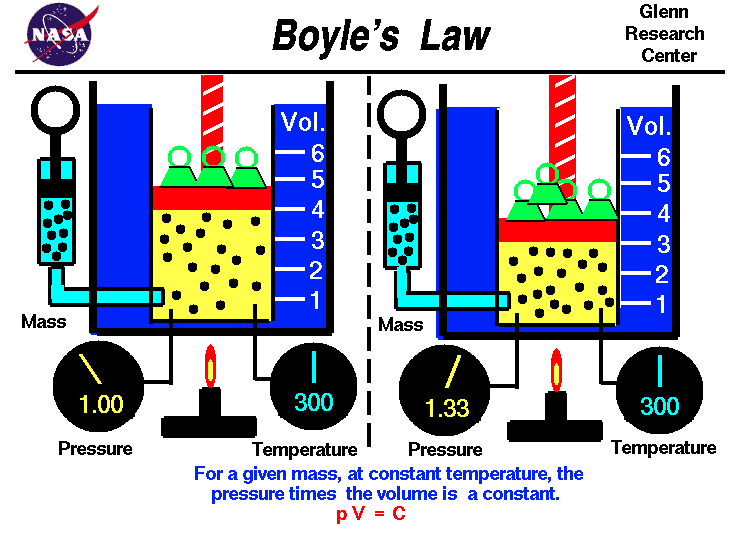
CFR Part 91.211 is the regulation governing use of supplemental oxygen. It’s based upon Boyle’s Law. Boyle’s Law states “the absolute pressure exerted by a given mass of an ideal gas is inversely proportional to the volume it occupies if the temperature and amount of gas remain unchanged within a closed system.”
In plain English, if we increase the volume of the air by decreasing its pressure, then the total number of molecules of oxygen in the atmosphere decreases.
 That number is a theoretical constant in the Earth’s atmosphere — 21% O2 on an International Standard Atmosphere (ISA) day of 59° Fahrenheit, at sea-level pressure of 14.7 psi. At 12,500 feet, less than two-thirds of ISA sea-level oxygen is available. At 14,000 feet, it’s 61%, and at 18,000 feet, it’s down to 52%.
That number is a theoretical constant in the Earth’s atmosphere — 21% O2 on an International Standard Atmosphere (ISA) day of 59° Fahrenheit, at sea-level pressure of 14.7 psi. At 12,500 feet, less than two-thirds of ISA sea-level oxygen is available. At 14,000 feet, it’s 61%, and at 18,000 feet, it’s down to 52%.
That’s why CFR Part 91.211 states if you’re flying above 12,500 feet, up to and including 14,000 feet, for more than 30 minutes, you have to use O2. Above 14,000 and up to and including 15,000 feet, all pilots must be on oxygen. Above that, everyone onboard must be breathing from a bag or a bottle. Under Part 91.211, the Bonanza pilot cruised legally at 12,500 feet. We were legal at 12,000 feet. But were we safe?
No, because when it comes to hypoxia, “legal” and “safe” ain’t always the same thing. We saw the signs. We knew at 12,000 feet at night it was odd not to need a jacket or the heater.
The Bonanza driver distinctly remembered thinking: “It was rather warm at altitude. This would have raised the density altitude even further.”
But like several other pilots reporting hypoxia-related incidents, we failed to heed Boyle’s Law. Or put another way, “It’s the density altitude, stupid.”
The L39C pilot ultimately managed to switch to his emergency 100% oxygen supply and land safely. When he took off again, he realized his speech was still slurred, so he wisely turned around, landed and spent the night recuperating.
We were less sanguine. We thought an hour on the ground restoring ourselves with coffee was sufficient. We pressed on, though at a much lower altitude. We ended our journey safely. However, the next day I slept 14 hours straight. My copilot suffered a prolonged headache.
The Bonanza pilot recovered enough after descending to a lower altitude to land safely at his destination.
And the flight crew of the G-III? They had the good sense to impose an immediate and permanent ban on the owner ever entering the flight deck again.
Source: http://generalaviationnews.comHypoxia, Part 1